
INTRODUCTION TO CARDIOVASCULAR SYSTEM
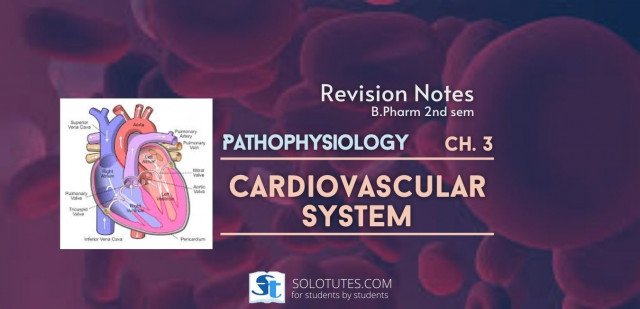
The heart is a muscular organ about the size of a closed fist located in the chest between the lungs behind the sternum and above the diaphragm. It is surrounded by pericardium. On its superior end, the base of the heart is attached to the aorta, pulmonary arteries and veins, and the vena cava. The inferior tip of the heart, known as the apex, rests just superior to the diaphragm. The base of the heart is located along the body’s midline with the apex pointing toward the left side.
Because the heart points to the left, about 2/3 of the heart’s mass is found on the left side of the body and the other 1/3 is on the right. The heart is the pump that is responsible for maintaining adequate circulation of oxygenated blood around the vascular network of the body. It takes in deoxygenated blood through the veins and delivers it to the lungs for oxygenation before pumping it into the various arteries.
Functions of Cardiovascular System
The cardiovascular system has three major functions: transportation, protection, and regulation of the body’s homeostasis.
Transportation: The cardiovascular system transports blood to almost all of the body’s tissues. The blood delivers essential nutrients and oxygen and removes wastes and carbon dioxide to be processed or removed from the body. Hormones are transported throughout the body via the blood’s liquid plasma.
Regulation: The cardiovascular system is instrumental in the body’s ability to maintain homeostatic control of several internal conditions.
The Circulatory Pump: The heart is a four-chambered “double pump”, where each side (left and right) operates as a separate pump. The left and right sides of the heart are separated by a muscular wall of tissue known as the septum of the heart.
Regulation of Blood Pressure: Several functions of the cardiovascular system can control blood pressure. Certain hormones along with autonomic nerve signals from the brain affect the rate and strength of heart contractions. Greater contractile force and heart rate lead to an increase in blood pressure. Blood vessels can also affect blood pressure.
Notes
1. ISCHAEMIC HEART DISEASE NOTES
ISCHAEMIC HEART DISEASE
Ischaemic heart disease (IHD) is defined as 'acute or chronic form of a cardiac disability arising from imbalance between the myocardial supply and demand of oxygenated blood'.
The alternate term coronary artery disease (CAD) is used synonymously with IHD. Depending on the rate and severity of coronary artery narrowing and the myocardial response, one of four syndromes may develop.
• Angina pectoris (Chest pain),
• Acute myocardial infarction,
• Chronic ischemic heart disease with congestive heart failure,
- Sudden cardiac death.
Etiology
The most common cause of ischemic heart disease is a reduction in coronary arterial blood supply due to atherosclerosis of the coronary arteries. Factors that contribute to the development of ischaemic heart disease are similar to those responsible for atherosclerosis in general, and include: Hypertension, diabetes mellitus, smoking, high cholesterol, high levels of low density lipoprotein, and genetic factors and non-atherosclerotic causes are vasospasm, coronary artery stenosis, inflammation of coronary arteries, thrombotic disease, trauma, aneurysms and compression.
Pathogenesis
Symptomatic ischemic heart disease is typically associated with a critical stenosis, defined as a 75% or greater reduction in the lumen of one or more coronary arteries by atherosclerotic plaque. With this level of fixed obstruction, the augmented coronary blood follow that may occur as a result of compensatory coronary vasodilation is insufficient to meet even moderate increase in myocardial oxygen demand. In addition to chronic, fixed atherosclerotic plaques, various superimposed lesions also play an important role in the development of myocardial ischemia. These include —
1. Acute changes in the morphology of chronic atherosclerotic plagues include fissuring, haemorrhage into the plaque, and plaque rupture with embolization of atheromataous debris into distal coronary vessels. In addition to causing enlargement of the plaque, local disruption of plaque increases the risk of platelet aggregation and thrombosis at the site.
2. Local plated aggregation in the coronary arteries has been documented in patients with unstable angina pectoris and in patients who undergo sudden cardiac death. Both mechanical occlusion of small blood vessels by small platelet aggregates and coronary vasospasm induced by mediators released from the platelet aggregates may contribute to myocardial ischemia.
3. Coronary artery thrombosis is almost always associated with a severe atherosclerotic plaque. Local disruption of atheromataous plaques plays an important role in the development of thrombi by exposing thrombogenic, lipid rich plaque debris to the blood.
4. Coronary artery spasm usually occurs in patients with at least some pre-existing atherosclerosis. It has been associated with one particular type of angina pectoris, termed Prinzmental’s (variant) angina.
Clinical Manifestations
Depending on the rate and severity of coronary artery narrowing and the myocardial response, one of four syndromes may develop.
1. Angina pectoris (Chest pain),
2. Acute myocardial infarction,
3. Chronic ischemic heart disease with congestive heart failure,
4. Sudden cardiac death.
Prevention
Fatty diet, smoking, sedentary lifestyle and stress should be avoided, as they are the main causes of Ischemic heart diseases. Avoiding food rich in saturated fats is important to reduce lipid levels in the blood and to prevent arteriosclerosis. Adequate regular exercise is also essential. Cholesterol and hypertension should be kept under good control with proper treatment.
Treatment
Organic Nitrates: These stimulates the intracellular cyclic-GMP, which results in vascular smooth muscle relaxation of both arterial and venous vasculature. e.g. Isosorbide dinitrate.
β-Blockers: β-Blockers act by reducing cardiac work and O2 consumption. e.g. Propranolol, Atenolol.
Calcium Channel Blockers: Calcium antagonist inhibits the passage of calcium ions through voltage-dependent L-type calcium channels in cell membranes in the heart and vascular smooth muscle as well as some other excitable tissues. e.g. Amlodipine Nifedipine.
Statins: IHD is also due to the increased cholesterol levels. Statins are used to reduce the cholesterol levels in hyper- cholesterolemia. Statins are the HMG-CoA reductase inhibitors. e.g. Atorvastatin, Rusvastatin.
Aspirin: Aspirin improves the rate of survival in patients with acute myocardial infarction and reduces the risk of myocardial infarction in patients with unstable angina, and after recovery from myocardial infarction.
Angina Pectoris
Angina pectoris is a clinical syndrome of Ischemic heart disease (IHD) resulting from transient myocardial ischaemia if the heart muscle does not get as much blood as it needs. This usually happens because one or more of the heart's arteries is narrowed or blocked. It is characterised by paroxysmal pain in the substernal or precordial region of the chest which is aggravated by an increase in the demand of the heart and relived by a decrease in the work of hear. Often, the pain radiates to the left arm, neck jaw or right arm.
Myocardial Infarction (Heart Attack)
Myocardial Infarction is a condition resulting from decreased blood and oxygen supply to the heart, causing cell death. The major cause is sudden blockage of coronary arteries.
Coronary arteries are blood vessels that supply the heart muscle with blood and oxygen. Blockage of a coronary artery deprives the heart muscle of blood and oxygen, causing injury to the heart muscle causing chest pain and chest pressure sensation.
Etiology
Myocardial infarction (MI) is the irreversible death (necrosis) of heart muscle which usually results from an imbalance in oxygen supply and demand, which is most often caused by plaque rupture with thrombus formation in an epicardial coronary artery, resulting in an acute reduction of blood supply to a portion of the myocardium.
Pathogenesis
1. Myocardial Ischaemia: Myocardial ischaemia is brought about by one or more of the following mechanisms:
(i) Diminised coronary blood flow e.g. in coronary artery disease shock.
(ii) Increased myocardial demand e.g. In exercise, emotions.
(iii) Hypertrophy of the heart without simultaneous increase of coronary blood flow e.g. in hypertension, valvular heart disease.
2. Role of platelets: Rupture of an atherosclerotic plaque exposes the subendothelial collagen to platelets which undergo aggregation, activation and release reaction. These events contribute to the build-up of the platelet mass that may give rise to emboli or initiate thrombosis.
3. Acute plaque rupture: In general, slowly developing coronary ischaemia from stenosis coronary atherosclerosis of high grade may not cause acute MI but continue to produce episodes of angina pectoris.
4. Non-atherosclerotic causes: About 10% cases of acute MI are caused by non-atherosclerotic factors such as coronary vasospasm, arteritis, coronary l stenosis embolism, thrombotic diseases, trauma and outside compression as already described.
Signs and Symptoms
Patients with typical MI may have the following symptoms in the days or even weeks preceding the event: Fatigue, Chest discomfort, Malaise.
Typical chest pain in acute MI has the following characteristics:
• Intense and unremitting for 30-60 minutes.
• Substernal, and often radiates upto the neck, shoulder, and jaw, and down the left arm.
• Usually described as a substernal pressure sensation that also may be characterized as squeezing, aching, burning, or even sharp.
- In some patients, the symptom is epigastric, with a feeling of indigestion or of fullness and gas.
Treatment
Emergency agents: Emergency agents are used in the process of reperfusion of the heart muscle. These agents basically help in relieving the severe heart pain, cause Vasodilatation to open the blocked artery, restore the oxygen supply and prevent the further damage of the heart muscle. These agents are morphine, oxygen, nitroglycerine, aspirin.
Anti-platelet agents: Anti-platelet medications prevent formation of blood clots in the arteries. In NSAID, aspirin inhibits cyclooxygenase-1 enzyme and thus prevents blood clotting by blocking the production of thromboxane A-2 by platelets, the chemical that causes platelets to clump.
Anti-coagulants: Anti-coagulant medications prevent growth of blood clots in the arteries. Anti-coagulants such as intravenous or subcutaneous heparin, subcutaneous low molecular weight heparin, and oral warfarin, prevent the formation of blood clots either by inhibiting the production of clotting factors or by interfering with the action of the clotting factors. e.g. Enoxaparin.
Clot-dissolving medications:
Fibrinolytic or thrombolytic agents are known as clot dissolving agents used to open blocked arteries and dissolve the existing clots.
β-adrenergic receptor blockers: β- blockers act by decreasing the workload of the heart. Decrease in the workload decreases the demand for oxygen by the heart and limits the amount of damage to the heart muscle.
2. Hypertension
HYPERTENSION
Hypertension is a chronic medical condition that arises when theblood pressure is abnormally high (greater than 140 mm of Hg systolic and 90 mm of Hg diastolic).
Hypertension occurs when the body’s smaller blood vessels (the arterioles) narrow, causing the blood to exert excessive pressure against the vessel walls and forcing the heart to work harder to maintain the pressure. Although the heart and blood vessels can tolerate increased blood pressure for months and even years, eventually the heart may enlarge (a condition called hypertrophy) and be weakened to the point of failure.
Hypertension risk factors include obesity, drinking too much alcohol, smoking and family history.
Blood pressure is actually a measure of two pressures, the systolic and the diastolic. The systolic pressure is the force that blood exerts on the artery walls as the heart contracts to pump the blood to the peripheral organs and tissues. The diastolic pressure is residual pressure exerted on the arteries as the heart relaxes between beats. A diagnosis of hypertension is made when blood pressure reaches or exceeds 140/90 mmHg (read as “140 over 90 millimetres of mercury”).
Types of Hypertension
There are two major types of hypertension and four less frequently found types.
1. Primary (Essential) Hypertension:
About 95% of people with high blood pressure have essential hypertension or primary hypertension. This condition has no identifiable medical cause. Elevated blood pressure usually begins to appear between age 30 and 50, but can begin at older ages.
Usually people with essential hypertension have no symptoms, but may
experience frequent headaches, tiredness, dizziness, or nose bleeds. Although the cause is unknown, but contributing factors for essential hypertension may be, obesity, smoking, alcohol, diet and inherited.
2. Secondary Hypertension: About 5%-10% of people with high blood pressure have secondary hypertension. This condition has definite cause; the most common cause of secondary hypertension is an abnormality in the arteries supplying blood to the kidneys. Other causes include airway obstruction during sleep, diseases and tumors of the adrenal glands, hormone abnormalities, thyroid disease, and too much salt or alcohol in the diet. Drugs can cause secondary hypertension, including OTC medications such as ibuprofen and pseudoephedrine.
Pathophysiology
Hypertension causes circulatory abnormalities: arteriolar resistance, increased large artery stiffness, and early or premature reflection of arterial pulse waves.
Increased resistance and vessel stiffness in younger hypertensive patients result from structural changes, including thinning and fracturing of elastin, increased collagen deposition, and increased wall thickness. These changes manifest primarily as a greater rise in systolic pressure greater than diastolic pressure.
There are many known conditions that can cause secondary hypertension. Regardless of the cause, arterial pressure becomes elevated either due to an increase in cardiac output, an increase in systemic vascular resistance, or both. When cardiac output is elevated, it is generally due to either increased neurohumoral activation of the heart or increased blood. Increased systemic vascular resistance is most commonly caused, at least initially, by increased sympathetic activation or by the effects of circulating vasoconstrictors (e.g., angiotensin II). Anatomic considerations, such as narrowing of the aorta (e.g., coarctation) or chronic changes in vascular structure (e.g., vascular hypertropy) can also cause or contribute to increased systemic vascular resistance. Renal artery disease can cause because of narrowing of the vessel lumen (stenosis).
Symptoms
High blood pressure usually causes no symptoms and high blood pressure often is labelled “the silent killer”. People who have high blood pressure typically do not know it until their blood pressure is measured.
Sometimes people with markedly elevated blood pressure may develop:
• Headache
• Dizziness
• Blurred vision
• Nausea and vomiting, and
• Chest pain and shortness of breath.
Prevention
Having high blood pressure can be prevented by eating healthily, maintaining a healthy weight, taking regular exercise, drinking alcohol in moderation and not smoking, reducing salt intake, managing stress.
3. Congestive Heart Failure
CONGESTIVE HEART FAILURE
Congestive Cardiac failure is a condition associated with heart disorders leading to impairment of the heart to supply sufficient blood to meet the body requirements. Cardiac Failure may be associated with the failure of the right or left ventricle or both. Cardiac failure causes the blood to move through the heart and body at a slower rate, leading to increased pressure in the heart. As a result, the heart is unable to pump enough oxygen and nutrients to meet the body's requirements. The heart chambers thus respond by stretching in order to hold more blood to pump through the body or by becoming more stiff and thickened. Such mechanism helps to keep the blood moving for a short while, but the heart muscle walls tend to weaken with time and then are unable to pump with enough strength.
The direct result of the reduced contractility of the cardiac muscles especially those of the ventricles, cause a decrease in the cardiac output and increase in the blood volume of the heart. This causes the kidneys to often respond by causing the body to retain fluid (water) and sodium, as the systemic blood pressure and the renal blood flow both are reduced. This results into building up of fluid in the arms, legs, ankles, feet, lungs or other organs causing oedema which makes the body congested, hence the name Congestive cardiac failure.
The term congestive heart failure is used for the chronic form of heart failure in which the patient has evidence of congestion of peripheral circulation and of lungs; CHF is the end result of various forms of serious heart diseases.
Etiology
There are many causes of congestive heart failure including:
1. Coronary artery disease leading to heart attacks and heart muscle weakness.
2. Primary heart muscle weakness from viral infections or toxins such as prolonged alcohol exposure.
3. Heart valve disease causing heart muscle weakness due to too much leaking of blood or heart muscle stiffness from a blocked valve, and Hypertension.
4. Rarer causes of heart failure include:
• Viral myocarditis (an infection of the heart muscle).
• Infiltrations of the muscle such as amyloidosis.
• HIV cardiomyopathy (caused by Human Immunodeficiency Virus).
• Connective tissue diseases such as Systemic lupus erythematosus.
• Abuse of drugs such as alcohol.
• Pharmaceutical drugs such as chemotherapeutic agents.
• Arrhythmias.
Pathogenesis
Heart failure may be caused by one of the following factors either singly or in combination.
1. Intrinsic Pump Failure: The most common and most important cause of heart failure is weakening of the ventricular muscle due to disease so that the heart fails to act as an efficient pump.
2. Increased workload on the heart:
Increased mechanical load on the heart results in increased myocardial demand resulting in myocardial failure. Increased load on the heart may be in the form of pressure load or volume load.
Types of Heart Failure
Congestive heart failure (CHF) is generally classified as systolic or diastolic heart failure and becomes progressively more common with increasing age. In addition, patients with risk factors for heart disease are more likely to develop congestive heart failure.
- Systolic Heart Failure
This condition occurs when the pumping action of the heart is reduced or weakened. A common clinical measurement is ejection fraction (EF). The ejection fraction is a calculation of how much blood is ejected out of the left ventricle (stroke volume) divided by the maximum volume remaining in the left ventricle at the end of diastole, or when the heart is relaxed after filling with blood.
2. Diastolic heart failure: This condition occurs when the heart can contract normally but is stiff, or less compliant, when it is relaxing and filling with blood. The heart is unable to fill with blood properly, which produces backup into the lungs and heart failure symptoms.
3. Acute heart failure: It is sudden and rapid development of failure following massive myocardial infarction, valve rupture, myocarditis etc. The sudden reduction in cardiac output, hypotension without edema is prominent features.
4. Chronic heart failure: It develops slowly with gradual reduction in cardiac output. It is commonly seen in slowly progressive valvular heart disease, systemic arterial hypertension, chronic obstructive pulmonary diseases etc.
Treatment
Treatment of Congestive Cardiac Failure is focused on improving the symptoms and preventing the progression of the disease. The major and often neglected form of treatment is lifestyle improvement, which includes:
1. Regulation of the salt and fluid intake: As the entire body suffers from congestion due to fluid accumulation and also that sodium leads to increased fluid accumulation in the body tissues, it is often recommended to restrict the sodium and fluid intake during the cardiac failure.
2. Exercise: It is recommended to do any activity which one can sustain for more than just a few minutes while your heart, lungs and muscles work overtime. Such an exercise is known as aerobic exercise
More in this Chapter..
ISCHAEMIC HEART DISEASE NOTES
Ischaemic heart disease (IHD) is defined as 'acute or chronic form of a cardiac disability arising from imbalance between the myocardial supply and de
4.5M Join the discussion.
Hypertension
Hypertension is a chronic medical condition that arises when theblood pressure is abnormally high (greater than 140 mm of Hg systolic and 90 mm of Hg
4.5M Join the discussion.
Congestive Heart Failure
Congestive Cardiac failure is a condition associated with heart disorders leading to impairment of the heart to supply sufficient blood to meet t
4.5M Join the discussion.













.jpg)






 संज्ञा
संज्ञा